Gastroenterology |
B57
|
Clinical Advice
Clinical Advice
We are happy to give clinical advice on weekdays via Cinapsis (a system that connects GPs to specialists) or for advice by email please contact us at ruh-tr.gastrosecs@nhs.net
Useful email contacts are also available here.
Cinapsis and the Gastro Secretaries inbox are checked on a daily basis during the working week by the departmental secretaries and enquiries distributed as appropriate. You may be able to find help with some queries in our FAQ section below.
The inbox is checked on a daily basis during the working week by the departmental secretaries and enquiries distributed as appropriate. You may be able to find help with some queries in our FAQ section below.
Frequently Asked Questions
Q: My patient has a low magnesium on PPI treatment, what can I do?
A: Options include lifestyle advice, alternative medication or magnesium supplements alongside PPI:
Lifestyle advice – dietary changes to increase magnesium consumption:
Magnesium is contained in a wide range of foods. In general, high-fibre foods (such as nuts, legumes, and leafy greens) contain magnesium, as well as various other sources such as some fortified cereals and electrolyte drinks. The recommended daily intake of magnesium is 300mg a day for men and 270mg a day for women aged 19 to 64 years.
BBC Good Food have a range of high-magnesium recipes for people to try.
Alternatives to PPIs:
Depending on the indication of the PPI, there are alternative options:
- Dyspepsia – non-pharmacological measures (such as weight loss, stopping smoking, dietary changes), antacids (such as Gaviscon), or H2 antagonists may be appropriate
- Gastric ulceration – for maintenance of remission a H2 antagonist may be appropriate. PPIs should be used preferentially during active ulceration due to increased safety and efficacy (1)
- Gastroprotection – the ongoing need for the medicine with high risk of GI bleeds/ulceration should be reviewed and discontinued if possible
Long-term PPI use should be reviewed and stepped down as appropriate, as per
BSW formulary guidelines
Long-term magnesium supplements:
Magnesium glycerophosphate is licensed for prevention of recurrence of magnesium deficit at a dose of 24mmol (97.2mg). Patients should be encouraged to buy supplements over the counter; a dose of under 400mg a day is unlikely to cause harm. Acute hypomagnesaemia should still be treated as per local or national guidance.
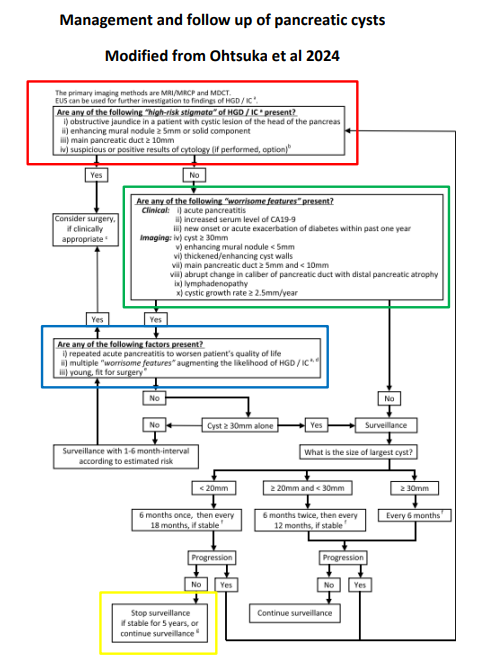
Q. My patient has been found to have a pancreatic cyst, they have asked if they will need a further scan, and where they might read more about it?
A. We have information available for patients here:
RUH Guidance for pancreatic cyst
Surveillance is delivered according to the guidance of the BRI Regional HPB team found here.
Q. My patient has been found to a gallbladder polyps – how do I determine the appropriate surveillance?
A. The RUH has published Gall Bladder Polyp Management Guidance; this approach is based on the current revised European guidance and can be reviewed here:
RUH Guidance for Gall Bladder Polyp Management
Q. Do patients with a positive TTG antibody need to have a small bowel biopsy to confirm the diagnosis of Coeliac disease?
A. Yes. All patients should have histological confirmation of the diagnosis. It is best to refer initially for an endoscopy rather than to the outpatient clinic. The patient should be advised to be on a normal wheat containing diet for six weeks prior to the endoscopy. Shorter periods of including gluten in the diet are acceptable if this is all the patient can manage but may lead to less reliable results.
Q. How do I monitor my patient on IBD medications under shared care?
A. See below:
RUH Guidance for Monitoring of IBD Medications
Q. My patient with an enteral tube has a tube-related concern?
A. RUH enteral tube information:
Enteral Tube Problems - Information for patients, nursing and medical staff
Q. Should this patient with a family history of colon cancer have colonoscopy screening?
A. The British Society of Gastroenterology's current recommendations for screening individuals with a family history of colon cancer are available via this link:
Guidelines for the management of hereditary colorectal cancer*
*Note: On page 8 of the document linked above is a list of the categories of risk and an image advising what screening is advised.
Q. My patient has IBD, they have presented with a flare. Where can I seek advice?
A. We have information available for GPs managing IBD patients below:
Alternatively, you can contact the gastroenterology team via Cinapsis - e.g. if the pathway hasn't helped.
Patients can contact the IBD helpline on: 01225 825598 between 8- 11 Monday to Friday.
Q. I have a patient with IBD asking about Coronavirus?
A. See the documents below.
We would recommend this resource:
Coronavirus (COVID-19) advice for people with IBD