
Breast Unit
Needle Localised wide local excision
Needle Localised Wide Local Excision of Breast Tumour
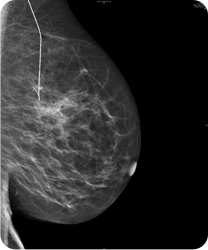 Mammogram showing the localisation wire to guide the surgeon at the time of surgery | On this page: The Operation Complications After Care |
The Operation
This operation involves removal of the breast tumour (as well as some of the lymph nodes in the armpit if required).
As the tumour cannot be clinically felt, we need to ask the Radiologist to accurately locate the tumour before surgery.
On the morning of the operation a scan will be undertaken in the Breast Unit and a guide wire inserted into the breast under ultrasound or ‘x-ray' guidance. Local anaesthetic is used to minimise any discomfort.
Later on that day the main operation will be undertaken under general anaesthetic. Through an incision on the breast the surgeon will remove the guide wire, the tumour and a rim of surrounding breast tissue.
The tissue will then be sent off to the laboratory to be analysed by the pathologists.
The operation takes in the region of 60 - 90 minutes to perform and the patient should be able to go home either on the same day or one day following the operation.
Complications
This is not a big or a difficult operation, although the breast may become quite bruised and swollen following the operation. In the long run it may also alter the size, shape and the contour of the breast somewhat, although we would hope that this would not be too marked.
Most patients do not have complications following this operation, but a small percentage of people may have them. These include the possibility of a wound infection or bleeding into the wound to form either a haematoma or extensive bruising.
After Care
Following discharge from the hospital a further appointment is made to come back to the breast unit to check the wounds and to discuss what has been found down the microscope and what further treatments are necessary to reduce the chances of the tumour coming back in the future.
As long as we find that the tumour has been adequately excised then patients are normally offered a course of radiotherapy to the breast to reduce the risk of local recurrence of the tumour in the years to come.
There is a chance that the pathologist might find that the tumour is larger down the microscope than we had anticipated. If that was the case then perhaps the margin of excision would be insufficient and we would suggest further surgery to her breast to achieve an adequate margin of excision. The chances of this happening would be approximately in the region of 20 – 30%.
Also See:
Wide Local Excision (Lumpectomy)
Axillary Lymph Node Dissection
Mastectomy without reconstruction